



Volume -
3 , - : 15-18 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Clinical Features of Breast Cancer in Elderly Women. 3 https://doi.org/10.58209/gmjm.2.1.15
URL: http://daneshafarand.org/article-1-197-en.html
URL: http://daneshafarand.org/article-1-197-en.html
| Abstract (HTML) (2423 Views)
Full-Text: (480 Views)
Introduction
Breast cancer is the most common malignancy in women worldwide and the second leading cause of death due to cancer in women. In Iran, about 17% of all cancers are related to breast cancer [1], which ranks first among Iranian women. Age is one of the biggest risk factors for developing new cases of breast cancer. About 50% of breast cancers occur in women 65 years and older and 35% after 70 years. The most common pathology subtype of all ages is duodenal carcinoma [2].
In recent decades, the incidence of breast cancer in people over the age of 70 has increased as life expectancy has increased [3]. There may be differences in the biology and clinical outcome of breast cancer by age (Figure 1). Doctors consider age as an important factor in treating patients. On the other hand, underlying and associated diseases affect the choice of treatment; The risk of mortality due to underlying diseases is 20 times higher in patients with breast cancer [4].
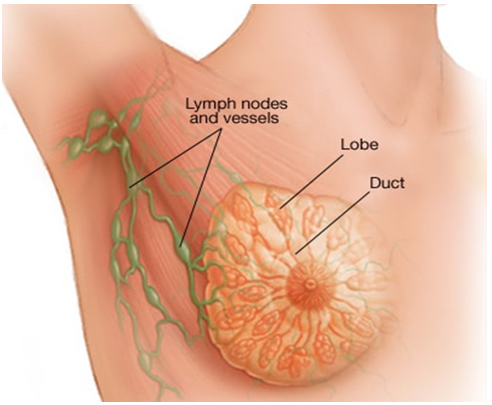
Figure 1) Breast cancer
Overall, studies show that older patients with breast cancer receive fewer treatments for breast cancer than younger patients. Today, there is no conclusive evidence of what is the best treatment for elderly patients and one of the reasons is the different factors and clinical characteristics in this age group of patients [5, 6].
Treatment decisions should not be based on age alone. Therefore, the aim of this study was to evaluate the status of breast cancer patients over 70 years of age in terms of clinical and pathological aspects in the clinics of hospitals in Tabriz (affiliated to Tabriz University of Medical Sciences) in order to investigate the effect of these characteristics on treatment.
Instrument and Methods
Study design
In this multicenter, retrospective and descriptive study, 2723 cases of women with breast cancer referred to oncology clinics affiliated to Tabriz University of Medical Sciences (Shahid Madani - Ghazi Tabatabai and Imam Reza) in a period of ten years leading to The year 2020 was evaluated. The samples were census and all files were evaluated according to the inclusion criteria.
Inclusion and exclusion criteria
One-hundred eighty three over 70 years old females with breast cancer were included in the study. Exclusion criteria also included files with incomplete and illegible information.
Procedure
The information in each file was recorded in the data collection form created for this purpose. This information includes: age, family history, personal history of other cancers, body mass status, type of tumor pathology, clinical stage of the tumor, status of hormone receptors and HER2 protein of the tumor, type of surgery, type of adjuvant treatment (radiotherapy, chemotherapy, hormone therapy) It was also extracted from the files.
Data analysis
Data were analyzed using SPSS 20 software. As the mentioned information was reported descriptively, no statistical test was used for this study.
Ethical considerations
This study has been approved by the ethics committee of Tabriz University of Medical Sciences (IR.TBZMED.REC.1398.151). Since this study is retrospective, the ethical approval of this project in the ethics committee of Tabriz University of Medical Sciences was considered as patients' consent to participate in this study. On the other hand, patients' personal information was kept secret and was not used.
Findings
The number of women with breast cancer who were older than 70 years was 107 (58.4%) of patients aged 75-70 years and 76 patients (41.3%) were older than 75 years. The mean age of the patients was 75.12±3.89 years. The age range of all patients was between 70 and 85 years.
118 patients (65.2%) were housewives, 153 urban patients (85.5%) and 160 patients (89.4%) were Azeri speakers. From all participants; Body mass index information available to 133 patients; 56 (42.10%) of them had normal body mass index, 40 (30.07%) were overweight and 26 (19.55%) were obese. Eleven patients (8.27%) were also thin. Also, the average body mass index in patients was 25.48±4.22.
125 patients (78.62%) had no family history of cancer and 34 patients (21.38%) also had a family history of cancer. The most common family history of cancer was breast cancer (34.6%). Patients (3.16%) had secondary cancer, of which two patients had endometrial cancer, one skin cancer patient, one lung cancer patient and one patient with multiple myeloma with breast cancer.
Seventy-six cases (53.32%) of the masses were on the left and 66 cases (46.48%) were on the right. In this study, pathological information was available from 161 women over 70 years of age with breast cancer. %) And Comedo (0.6%). The rate of tumors with positive estrogen receptor was 65.8% and tumors with positive progesterone receptor were 59.85%.
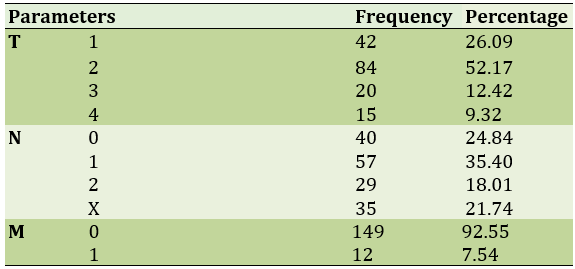
Patients with HER2-negative tumor (0 or +1) were 89 cases (64.5%), HER2-positive tumor (+3) were 29 cases (21%), and ambiguous HER2 tumor (2+) were 20 cases (14.49%). In the study of 161 patients, 57 patients (35.40%) were N1 patients and 149 patients (92.55%) were M0 and 84 patients (52.17%) were T2 patients (Table 1).
Table 1) Evaluation of mass size (T), lymph node (N) and metastasis (M)
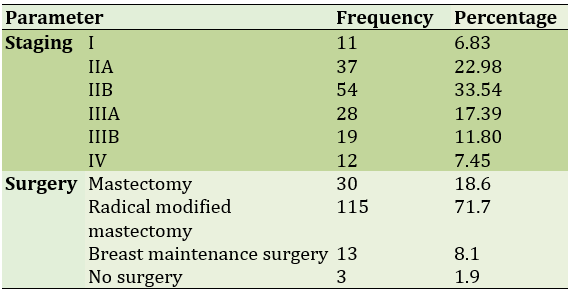
Most patients (33.54%) were in stage IIB and only 11 people (6.83%) were in stage I. The most common type of radical surgery was modified mastectomy (71.4%; Table 2).
Table 2) Frequency of the disease stage and type of surgery
Eighty-three patients (51.6%) received tamoxifen, 12 (7.5%) received letrozole, 112 (70%) received chemotherapy, and 88 (54.7%) received radiotherapy. The most common chemotherapy regimen used in patients with CAF (cyclophosphamide, adriamycin, 5-fluorosil) was 55.4%, followed by cyclophosphamide methotrexate (33.9%) and Taxane, adriamycin, cyclophosphamide and taxan in 10.7% of patients.
In the present study, there were 40 non-metastatic lymph node-negative patients, of which 9 (22.5%) had no estrogen receptor and 31 (77.5%) had estrogen receptor. The most systemic treatment received in patients without estrogen receptor was only chemotherapy (77.8%) and in patients with estrogen receptor tumor was only hormone therapy (54%).
In 88 non-metastatic patients, there were 90 lymph nodes positive, of which 33 (37.5%) had no estrogen receptor and 55 (62.5%) had estrogen receptor. The most systemic treatment in patients with estrogen receptor-free tumor was chemotherapy (81.8%) and in patients with estrogen receptor tumor, chemotherapy plus hormone therapy (58.2%).
Discussion
Breast cancer is the most common malignancy in women worldwide and the most common cause of death due to cancer in women [7]. Age is one of the biggest risk factors for developing new breast cancers. About 50% of breast cancers occur in women 65 and older and 35% after 70 years [8].
In the present study, which examined 183 cases of women with breast cancer over the age of 70, most patients were between the ages of 70 and 75, with a mean age of 75.12 ± 3.89 years. The mean age in other studies was not significantly different from the present study. In a similar study [9], the mean age of patients was 75 years. In the study ... and colleagues, the average age was 76 years and in the study ... and colleagues, the average age was 74 years.
In the present study, in the study of body mass index, the highest frequency of patients in terms of body mass index was in individuals with normal body mass index. In addition, 34 patients had a family history of cancer, which was more than breast cancer. In the study [10] the average body mass index in the study population was 45, which was similar to the present study. Also in the study [11] 2% of patients had a family history of breast cancer and 9% had a family history of other cancers, which was different from the present study.
In the present study, the frequency of estrogen and progesterone receptors in the tumor was 65.8% and 59.85%, respectively, and the frequency of patients with HER2-negative tumor was 64.5 and HER2-positive tumor was 21%, and the frequency of patients with invasive ductal carcinoma was 89.4%. In a similar study, 86% of patients had estrogen receptors in the tumor and 72% of patients had invasive ductal carcinoma, which was similar to the present study. In another study, 86% of patients had invasive carcinoma, 67% had an estrogen receptor tumor, and 58% had a progesterone receptor tumor. In another study, the most common pathological findings in women of premenopausal age were fibroadenoma and in postmenopausal age were ductal carcinoma, which was similar to the results of the study population. In several other studies, breast tumors over the age of 70 were more positive for the hormone receptor type [12, 13].
In the present study, most of the patients were in stage II, which was consistent with the results of a similar study in which 18% of patients were in stage I, 57% of patients were in stage II, and 25% of patients were in stage III. In the present study, most of the surgeries performed in patients underwent radical mastectomy, which is consistent with the results of several studies in this field [14].
In the present study, 59% of patients received hormone therapy, 70% received chemotherapy and 54% received radiotherapy, which was significantly different from the results of several studies. In the study, hormone therapy was performed in 18% of patients, chemotherapy in 12% of patients, and radiotherapy in 25% of patients, and these differences are probably due to different clinical stages [15, 16].
One of the limitations of this study was the lack of disease registration systems and consequently the lack of access to information of all patients. One of the strengths of the present study was the 10-year study of patients in three oncology centers and thus the possibility of access to a sufficient number of samples. It is suggested that in future studies, the relationship between clinical characteristics and the type of treatment and survival of breast cancer patients over 70 years of age should be investigated.
Conclusion
It seems that the most common stage of the disease in elderly women and over 70 years is type IIB, which is also more common in these elderly women with breast cancer; Therefore, it is necessary to pay attention to these points in treatment planning.
Acknowledgements: None declared by the authors.
Ethical Permission: None declared by the authors.
Conflicts of Interests: None declared by the authors.
Funding/Support: None declared by the authors.
Breast cancer is the most common malignancy in women worldwide and the second leading cause of death due to cancer in women. In Iran, about 17% of all cancers are related to breast cancer [1], which ranks first among Iranian women. Age is one of the biggest risk factors for developing new cases of breast cancer. About 50% of breast cancers occur in women 65 years and older and 35% after 70 years. The most common pathology subtype of all ages is duodenal carcinoma [2].
In recent decades, the incidence of breast cancer in people over the age of 70 has increased as life expectancy has increased [3]. There may be differences in the biology and clinical outcome of breast cancer by age (Figure 1). Doctors consider age as an important factor in treating patients. On the other hand, underlying and associated diseases affect the choice of treatment; The risk of mortality due to underlying diseases is 20 times higher in patients with breast cancer [4].
Figure 1) Breast cancer
Overall, studies show that older patients with breast cancer receive fewer treatments for breast cancer than younger patients. Today, there is no conclusive evidence of what is the best treatment for elderly patients and one of the reasons is the different factors and clinical characteristics in this age group of patients [5, 6].
Treatment decisions should not be based on age alone. Therefore, the aim of this study was to evaluate the status of breast cancer patients over 70 years of age in terms of clinical and pathological aspects in the clinics of hospitals in Tabriz (affiliated to Tabriz University of Medical Sciences) in order to investigate the effect of these characteristics on treatment.
Instrument and Methods
Study design
In this multicenter, retrospective and descriptive study, 2723 cases of women with breast cancer referred to oncology clinics affiliated to Tabriz University of Medical Sciences (Shahid Madani - Ghazi Tabatabai and Imam Reza) in a period of ten years leading to The year 2020 was evaluated. The samples were census and all files were evaluated according to the inclusion criteria.
Inclusion and exclusion criteria
One-hundred eighty three over 70 years old females with breast cancer were included in the study. Exclusion criteria also included files with incomplete and illegible information.
Procedure
The information in each file was recorded in the data collection form created for this purpose. This information includes: age, family history, personal history of other cancers, body mass status, type of tumor pathology, clinical stage of the tumor, status of hormone receptors and HER2 protein of the tumor, type of surgery, type of adjuvant treatment (radiotherapy, chemotherapy, hormone therapy) It was also extracted from the files.
Data analysis
Data were analyzed using SPSS 20 software. As the mentioned information was reported descriptively, no statistical test was used for this study.
Ethical considerations
This study has been approved by the ethics committee of Tabriz University of Medical Sciences (IR.TBZMED.REC.1398.151). Since this study is retrospective, the ethical approval of this project in the ethics committee of Tabriz University of Medical Sciences was considered as patients' consent to participate in this study. On the other hand, patients' personal information was kept secret and was not used.
Findings
The number of women with breast cancer who were older than 70 years was 107 (58.4%) of patients aged 75-70 years and 76 patients (41.3%) were older than 75 years. The mean age of the patients was 75.12±3.89 years. The age range of all patients was between 70 and 85 years.
118 patients (65.2%) were housewives, 153 urban patients (85.5%) and 160 patients (89.4%) were Azeri speakers. From all participants; Body mass index information available to 133 patients; 56 (42.10%) of them had normal body mass index, 40 (30.07%) were overweight and 26 (19.55%) were obese. Eleven patients (8.27%) were also thin. Also, the average body mass index in patients was 25.48±4.22.
125 patients (78.62%) had no family history of cancer and 34 patients (21.38%) also had a family history of cancer. The most common family history of cancer was breast cancer (34.6%). Patients (3.16%) had secondary cancer, of which two patients had endometrial cancer, one skin cancer patient, one lung cancer patient and one patient with multiple myeloma with breast cancer.
Seventy-six cases (53.32%) of the masses were on the left and 66 cases (46.48%) were on the right. In this study, pathological information was available from 161 women over 70 years of age with breast cancer. %) And Comedo (0.6%). The rate of tumors with positive estrogen receptor was 65.8% and tumors with positive progesterone receptor were 59.85%.
Patients with HER2-negative tumor (0 or +1) were 89 cases (64.5%), HER2-positive tumor (+3) were 29 cases (21%), and ambiguous HER2 tumor (2+) were 20 cases (14.49%). In the study of 161 patients, 57 patients (35.40%) were N1 patients and 149 patients (92.55%) were M0 and 84 patients (52.17%) were T2 patients (Table 1).
Table 1) Evaluation of mass size (T), lymph node (N) and metastasis (M)
Most patients (33.54%) were in stage IIB and only 11 people (6.83%) were in stage I. The most common type of radical surgery was modified mastectomy (71.4%; Table 2).
Table 2) Frequency of the disease stage and type of surgery
Eighty-three patients (51.6%) received tamoxifen, 12 (7.5%) received letrozole, 112 (70%) received chemotherapy, and 88 (54.7%) received radiotherapy. The most common chemotherapy regimen used in patients with CAF (cyclophosphamide, adriamycin, 5-fluorosil) was 55.4%, followed by cyclophosphamide methotrexate (33.9%) and Taxane, adriamycin, cyclophosphamide and taxan in 10.7% of patients.
In the present study, there were 40 non-metastatic lymph node-negative patients, of which 9 (22.5%) had no estrogen receptor and 31 (77.5%) had estrogen receptor. The most systemic treatment received in patients without estrogen receptor was only chemotherapy (77.8%) and in patients with estrogen receptor tumor was only hormone therapy (54%).
In 88 non-metastatic patients, there were 90 lymph nodes positive, of which 33 (37.5%) had no estrogen receptor and 55 (62.5%) had estrogen receptor. The most systemic treatment in patients with estrogen receptor-free tumor was chemotherapy (81.8%) and in patients with estrogen receptor tumor, chemotherapy plus hormone therapy (58.2%).
Discussion
Breast cancer is the most common malignancy in women worldwide and the most common cause of death due to cancer in women [7]. Age is one of the biggest risk factors for developing new breast cancers. About 50% of breast cancers occur in women 65 and older and 35% after 70 years [8].
In the present study, which examined 183 cases of women with breast cancer over the age of 70, most patients were between the ages of 70 and 75, with a mean age of 75.12 ± 3.89 years. The mean age in other studies was not significantly different from the present study. In a similar study [9], the mean age of patients was 75 years. In the study ... and colleagues, the average age was 76 years and in the study ... and colleagues, the average age was 74 years.
In the present study, in the study of body mass index, the highest frequency of patients in terms of body mass index was in individuals with normal body mass index. In addition, 34 patients had a family history of cancer, which was more than breast cancer. In the study [10] the average body mass index in the study population was 45, which was similar to the present study. Also in the study [11] 2% of patients had a family history of breast cancer and 9% had a family history of other cancers, which was different from the present study.
In the present study, the frequency of estrogen and progesterone receptors in the tumor was 65.8% and 59.85%, respectively, and the frequency of patients with HER2-negative tumor was 64.5 and HER2-positive tumor was 21%, and the frequency of patients with invasive ductal carcinoma was 89.4%. In a similar study, 86% of patients had estrogen receptors in the tumor and 72% of patients had invasive ductal carcinoma, which was similar to the present study. In another study, 86% of patients had invasive carcinoma, 67% had an estrogen receptor tumor, and 58% had a progesterone receptor tumor. In another study, the most common pathological findings in women of premenopausal age were fibroadenoma and in postmenopausal age were ductal carcinoma, which was similar to the results of the study population. In several other studies, breast tumors over the age of 70 were more positive for the hormone receptor type [12, 13].
In the present study, most of the patients were in stage II, which was consistent with the results of a similar study in which 18% of patients were in stage I, 57% of patients were in stage II, and 25% of patients were in stage III. In the present study, most of the surgeries performed in patients underwent radical mastectomy, which is consistent with the results of several studies in this field [14].
In the present study, 59% of patients received hormone therapy, 70% received chemotherapy and 54% received radiotherapy, which was significantly different from the results of several studies. In the study, hormone therapy was performed in 18% of patients, chemotherapy in 12% of patients, and radiotherapy in 25% of patients, and these differences are probably due to different clinical stages [15, 16].
One of the limitations of this study was the lack of disease registration systems and consequently the lack of access to information of all patients. One of the strengths of the present study was the 10-year study of patients in three oncology centers and thus the possibility of access to a sufficient number of samples. It is suggested that in future studies, the relationship between clinical characteristics and the type of treatment and survival of breast cancer patients over 70 years of age should be investigated.
Conclusion
It seems that the most common stage of the disease in elderly women and over 70 years is type IIB, which is also more common in these elderly women with breast cancer; Therefore, it is necessary to pay attention to these points in treatment planning.
Acknowledgements: None declared by the authors.
Ethical Permission: None declared by the authors.
Conflicts of Interests: None declared by the authors.
Funding/Support: None declared by the authors.
Article Type: Descriptive & Survey |
Subject:
Biotechnology
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |