



Volume -
3 , - : 73-76 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Effect of Aerobic and Anaerobic Fitness on Different Psychological Parameters in Children with Tic Disorder. 3 https://doi.org/10.58209/gmjm.3.2.73
URL: http://daneshafarand.org/article-1-224-en.html
URL: http://daneshafarand.org/article-1-224-en.html
Keywords: Aerobic Fitness, Anaerobic Fitness, Physical Injury Fears, Social Phobia, Obsessive-Compulsive, Tic syndrome
| Abstract (HTML) (4200 Views)
Full-Text: (617 Views)
Introduction
Tourette syndrome (TS) is known as a neurodevelopmental disorder in patients with motor and vocal tics for at least one year [1]. Tics are not serious disorders but transient disorders in childhood that influence children's development [2]. Tics are short and insignificant, such as blinking, grimacing head, nose twitching, mouth, and shoulder movements [1]. Tics are short, but these influence psychological performance in children and members of the family [2]. Children with tic disorders are faced with neuropsychiatric conditions, such as attention deficit hyperactivity disorder and obsessive-compulsive [3]. It was reported that 85% of anxiety disorders in children with tic disorders [3]. Parents and children commonly report distressed behaviors associated with faulted daily function and anxiety disorders [4]. Different strategies are used for decreasing psychological symptoms in patients with tic syndrome, such as drugs, physical activity, etc. The application of drugs has been faced with limitations due to their side effects [2]. Researchers are interested in using physical activity to alleviate psychological disorders. It was reported that using exercises alleviates diseases [5].
Physical activity is an appropriate strategy for the alleviation of adverse effects of disorders. Exercise is considered the first strategy for the prevention and management of disorders. Performing regular exercise causes physiological changes and adaptations in the human body by affecting hypothalamic-pituitary-adrenal (HPA) axis reactivity [6, 7]. The region has an important role in improving adaptive responses to physical and psychological stressors [8]. It was reported depressive and anxiety signs in patients with faults in the HPA [9]. Exercises are divided into aerobic and anaerobic exercises [10]. Aerobic and anaerobic exercises have different effects on the physiology of the body. It was reported that this type of exercise can appropriately affect mental indices [11]. Other studies did not find positive effects of physical activities on mental indices [12]. It was reported that the efficiency of anaerobic exercises in decreasing anxiety [13].
Seemingly, aerobic and anaerobic fitness can have positive effects on psychological function in children with motor tics. Psychological disorders are a part of tic syndrome that are not considered by the scientific community, but these influence children. To the best of our knowledge, no study has been conducted to evaluate the effect of aerobic and anaerobic fitness on psychological function in children with a tic disorder. This study was thus conducted to evaluate the effect of aerobic and anaerobic fitness on separation anxiety, generalized anxiety, social phobia, obsessive-compulsive behaviors, panic and agoraphobia, and physical injury fears in children with a tic disorder.
Materials and Methods
Ethics Statement
All the procedures used were in agreement with the local Ethical Committee of the Physical Education Review Board of Islamic Azad University, Kermanshah-Iran (No. of permission, IAUKI-13401). We collected consent from parents of all the subjects before their children participated. Not only children but also their parents completed consent forms.
Study procedure
This randomized controlled trial was conducted for 12 weeks in children with motor tics. Forty-five girl children were randomly assigned into 3 groups: 1) the Aerobic group, where children exercised aerobic fitness for 12 weeks; 2) the Anaerobic group, where children exercised anaerobic exercises for 12 weeks; and 3) the Control group, where children did not receive any training.
Participants
Forty-five children ranging from 9 to 11 years (10.78±1.24) were studied in this study and completed evaluations at post-test. The flowchart of the study is illustrated in Figure 1. Body weight (in shorts and t-shirt) and height (without shoes) were investigated by an electronic scale and converted to body mass index (BMI). Children were randomly selected from local elementary schools in the Kermanshah Province, West region. The inclusion criteria were as follows; 1) Consent of children for participation in the study, 2) Children aged between 10 and 12 years of age, 3) Children had no medical condition that would affect study results or limit physical activity, 4) Children with tic severity >2 and 5) Children were not taking medication that would affect study results (e.g. antipsychotics). Exclusion criteria included: 1) Children did not have a tendency to participate in this study, 2) Children with tic severity <2, 3) Consumption of drugs that would affect study results or limit physical activity, 4) The use of antipsychotics, and 5) Non-participating in exercises for at least 2 meetings.
Yale Global Tic Severity Scale
The Yale global tic severity scale is a clinician-rated measure for tic severity over the last 7–10 days that has a stable factor structure and excellent psychometric properties. The motor and tics are rated at a 0–5 scale across 5 dimensions: number, frequency, intensity, complexity, and interference [14].
Exercise intervention
The exercise sessions were carried out after school and were conducted in consecutive sessions. Children were transported by bus to a training place in Kermanshah City. Instructors included master’s level physical educators, bachelor’s level exercise scientists, and other trained research staff who had at least some college education. In this study, we emphasized enjoyment and safety but no competition. The aerobic training program was designed using a cycle ergometer, triplicated a week, for 12 weeks, and for an initial period of 40 minutes [16]. The anaerobic training was performed using the method of “Interspaced Training [15]. In this study, parents completed Spence Children’s Anxiety Scale Child and Parent Versions in the pre-test (pre-interventions) and post-test (after 12-week exercises). The questionnaire included 38 items rated on a 4-point scale (0 to 3; never to always), and the SCAS-C includes six additional positive filler items. The SCAS-C/P comprises six subscales addressing Separation Anxiety (six items), Generalized Anxiety (six items), Social Phobia (six items), Obsessive–Compulsive Behaviors (six items), Panic and Agoraphobia (nine items), and Physical Injury Fears (five items).
Statistical Analysis
The present study was conducted in a 2×3 factorial arrangement with the effect of time (pre-test & post-test) and exercises (Control, Aerobic & Anaerobic) and their interaction. The data were reported as mean±SD and analyzed for the main effects of time and exercise and the interactions between time and exercise. The data were analyzed using SPSS 23 software. Comparisons between groups were conducted by the Sceffe test, and the T-test conducted paired-tests. Kolmogorov-Smirnov test was used to test the normality.
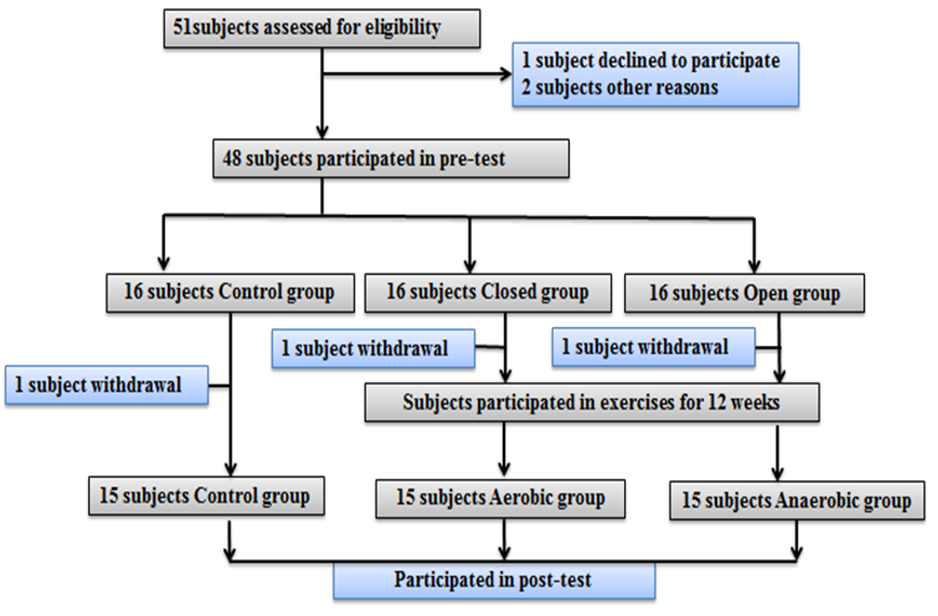
Figure 1. Flowchart of the study
Findings
Descriptive characteristics
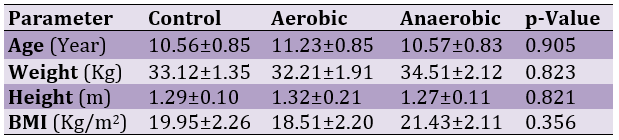
There were no significant differences between groups (p>0.05) according to age, weight, height, and BMI conditions.
Table 1. The subjects' characteristics
Yale Global Tic Severity Scale
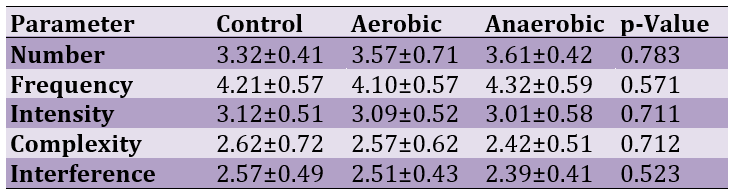
Table 2 presents our findings for five dimensions in the different groups. The results did not show significant differences between groups (p>0.05).
Table 2. Distribution of Yale global tic severity scale scores across participants
Normality
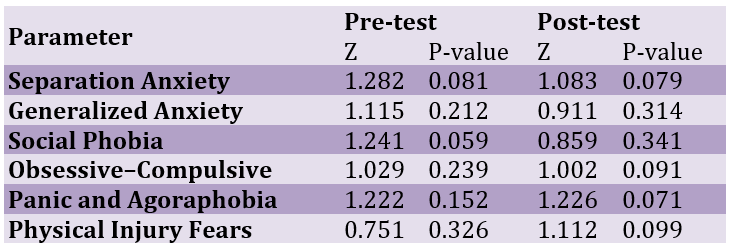
Table 3 shows the normality distribution results for all the parameters in the pre-test and post-test. The results showed that values higher than 0.05 meant normality.
Table 3. The results for normality status (all were normal)
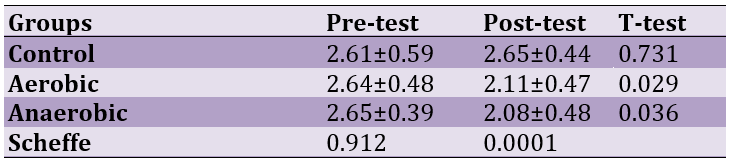
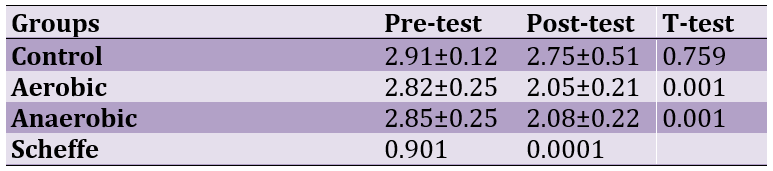
The effect of aerobic and anaerobic fitness on Separation Anxiety
The effect of aerobic and anaerobic fitness on Separation Anxiety for time (F(1, 44)=7.10; p=0.0009), fitness (F(2, 44)=5.41; p=0.001) and time × fitness interaction (F(1, 44)=6.12; p=0.001) were shown in Table 4. Scheffe test showed a significant difference between groups in the post-test (p=0.0001). The results showed that aerobic and anaerobic fitness decreased separation anxiety in the post-test (Table 4).
Table 4. The effect of aerobic and anaerobic fitness on Separation Anxiety in pre and post-Test
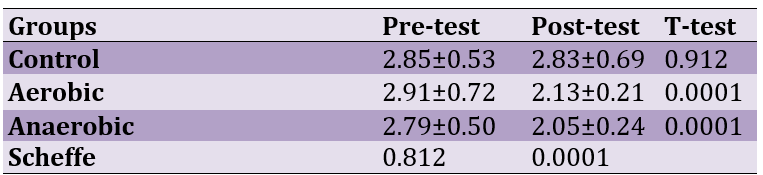
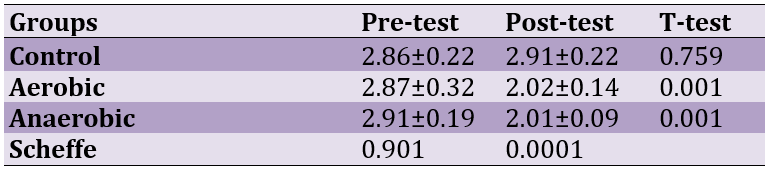
The effect of aerobic and anaerobic fitness on Panic and Agoraphobia
The effect of aerobic and anaerobic fitness on Panic and Agoraphobia for time (F(1, 44)=7.08; p=0.0001), fitness (F(2, 44)=7.22; p=0.0001) and time × fitness interaction (F(1, 44)=7.67; p=0.0001) were shown in Table 5. There was a significant response for the Scheffe test in the post-test (p=0.0001). The results showed that aerobic and anaerobic fitness reduced Panic and Agoraphobia (Table 5).
Table 5. Effect of Fitness on Panic and Agoraphobia in pre and post-Test
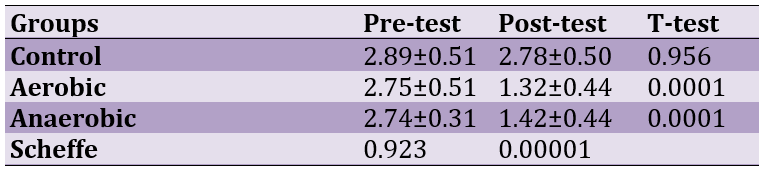
The effect of aerobic and anaerobic fitness on Physical Injury Fears
The effect of aerobic and anaerobic fitness on Physical Injury Fears for time (F(1, 44)=31.48; p=0.0001), fitness (F(2, 44)=15.48; p=0.0001) and time × fitness interaction (F(1, 44)=16.39; p=0.0001) were shown in Table 6. Scheffe test showed a significant difference between groups in the post-test (p=0.0001). Aerobic and anaerobic fitness decreased Physical Injury Fears (Table 6).
Table 6. Effect of skill exercises on Physical Injury Fears in pre and post-Test
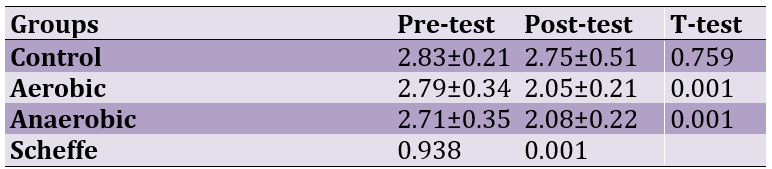
The effect of aerobic and anaerobic fitness on Generalized Anxiety
The effect of aerobic and anaerobic fitness on Generalized Anxiety for time (F(1, 44)=14.20; p=0.0001), fitness (F(2, 44)=21.18; p=0.0001), and time × fitness interaction (F(1, 44)=15.49; p=0.0001) were shown in Table 7. There was a significant response for the Scheffe test in the post-test (p=0.001).
Table 7. The effects of skill exercises on Generalized Anxiety in pre and post-Test
The effect of aerobic and anaerobic fitness on Social Phobia
The effect of aerobic and anaerobic fitness on Social Phobia for time (F(1, 44)=19.60; p=0.0001), fitness (F(2, 44)=21.45; p=0.0001), and time × fitness interaction (F(1, 44)=23.12; p=0.0001) were shown in Table 8. Significant responses were observed for the Scheffe test in the post-test (p=0.0001).
Table 8. The effects of skill exercises on aerobic and anaerobic fitness on Social Phobia in pre and post-Test
The effect of aerobic and anaerobic fitness on Obsessive–Compulsive
The effect of aerobic and anaerobic fitness on Social Phobia for time (F(1, 44)=21.20; p=0.0001), fitness (F(2, 44)=23.31; p=0.0001), and time × fitness interaction (F(1, 44)=19.75; p=0.0001) were shown in Table 9. Significant responses were observed for the Scheffe test in the post-test (p=0.0001).
Table 9. The effects of skill exercises on aerobic and anaerobic fitness on Obsessive–Compulsive in pre and post-Test
Discussion
The results showed that aerobic and anaerobic fitness had positive effects on decreasing psychological disorders in children with tic syndrome. No study has been found to show the effects of aerobic and anaerobic fitness on psychological parameters in children with motor tics. Conversely, Strohle et al. [16] assessed the effects of aerobic treadmill exercise on anti-panic and anxiolytic activity in patients with panic disorder and showed that anxiety was significantly higher in patients submitted to treadmill exercise. The results are in contrast with our findings. The reason for the difference between our findings and others could be attributed to physiological conditions. Parallel to our findings, Bandelow et al. [17] aerobic exercise decreased anxiety symptoms. In another study, Gomes da Silva [18] showed that physical activity affects attention, depression, anxiety, and overall well-being. Other studies showed that aerobic and anaerobic fitness improved neuropsychological and electrophysiological performances of working memory in preadolescent children [19]. An animal study assessed the effects of long-term wheel running on anxiety-like behavior in transgenic mice and showed decreased anxiety-like behavior [20]. It was reported that aerobic exercises have positive effects on the density of neural conveyors in the neural system and reduce muscular tension and hormone levels [20-25]. Other studies showed that aerobic exercises decrease the level of stress and anxiety by influencing the automatic neural system and decreasing anxiety and depression [25]. Aerobic fitness decreases cortisol levels and anxiety [26]. Kim et al. [27] investigated the responses of five participants to aerobic exercises and anaerobic exercises and showed that different fitness improved mental health and happiness, each with a different degree, which verifies the results of the present study. Other studies showed that aerobic and group activities are more effective for improving mental well-being compared to anaerobic and individual exercises [25].
Conclusion
Both fitness similarly decreased psychological disorders in children with tic syndrome. It can be suggested to use aerobic and aerobic fitness to decrease psychological disorders in patients with psychological disorders.
Acknowledgments: This work was supported by Islamic Azad University, Kermanshah Branch, Kermanshah, Iran.
Ethical Permission: None declared by the authors.
Conflicts of Interests: None declared by the authors.
Funding/Support: None declared by the authors.
Tourette syndrome (TS) is known as a neurodevelopmental disorder in patients with motor and vocal tics for at least one year [1]. Tics are not serious disorders but transient disorders in childhood that influence children's development [2]. Tics are short and insignificant, such as blinking, grimacing head, nose twitching, mouth, and shoulder movements [1]. Tics are short, but these influence psychological performance in children and members of the family [2]. Children with tic disorders are faced with neuropsychiatric conditions, such as attention deficit hyperactivity disorder and obsessive-compulsive [3]. It was reported that 85% of anxiety disorders in children with tic disorders [3]. Parents and children commonly report distressed behaviors associated with faulted daily function and anxiety disorders [4]. Different strategies are used for decreasing psychological symptoms in patients with tic syndrome, such as drugs, physical activity, etc. The application of drugs has been faced with limitations due to their side effects [2]. Researchers are interested in using physical activity to alleviate psychological disorders. It was reported that using exercises alleviates diseases [5].
Physical activity is an appropriate strategy for the alleviation of adverse effects of disorders. Exercise is considered the first strategy for the prevention and management of disorders. Performing regular exercise causes physiological changes and adaptations in the human body by affecting hypothalamic-pituitary-adrenal (HPA) axis reactivity [6, 7]. The region has an important role in improving adaptive responses to physical and psychological stressors [8]. It was reported depressive and anxiety signs in patients with faults in the HPA [9]. Exercises are divided into aerobic and anaerobic exercises [10]. Aerobic and anaerobic exercises have different effects on the physiology of the body. It was reported that this type of exercise can appropriately affect mental indices [11]. Other studies did not find positive effects of physical activities on mental indices [12]. It was reported that the efficiency of anaerobic exercises in decreasing anxiety [13].
Seemingly, aerobic and anaerobic fitness can have positive effects on psychological function in children with motor tics. Psychological disorders are a part of tic syndrome that are not considered by the scientific community, but these influence children. To the best of our knowledge, no study has been conducted to evaluate the effect of aerobic and anaerobic fitness on psychological function in children with a tic disorder. This study was thus conducted to evaluate the effect of aerobic and anaerobic fitness on separation anxiety, generalized anxiety, social phobia, obsessive-compulsive behaviors, panic and agoraphobia, and physical injury fears in children with a tic disorder.
Materials and Methods
Ethics Statement
All the procedures used were in agreement with the local Ethical Committee of the Physical Education Review Board of Islamic Azad University, Kermanshah-Iran (No. of permission, IAUKI-13401). We collected consent from parents of all the subjects before their children participated. Not only children but also their parents completed consent forms.
Study procedure
This randomized controlled trial was conducted for 12 weeks in children with motor tics. Forty-five girl children were randomly assigned into 3 groups: 1) the Aerobic group, where children exercised aerobic fitness for 12 weeks; 2) the Anaerobic group, where children exercised anaerobic exercises for 12 weeks; and 3) the Control group, where children did not receive any training.
Participants
Forty-five children ranging from 9 to 11 years (10.78±1.24) were studied in this study and completed evaluations at post-test. The flowchart of the study is illustrated in Figure 1. Body weight (in shorts and t-shirt) and height (without shoes) were investigated by an electronic scale and converted to body mass index (BMI). Children were randomly selected from local elementary schools in the Kermanshah Province, West region. The inclusion criteria were as follows; 1) Consent of children for participation in the study, 2) Children aged between 10 and 12 years of age, 3) Children had no medical condition that would affect study results or limit physical activity, 4) Children with tic severity >2 and 5) Children were not taking medication that would affect study results (e.g. antipsychotics). Exclusion criteria included: 1) Children did not have a tendency to participate in this study, 2) Children with tic severity <2, 3) Consumption of drugs that would affect study results or limit physical activity, 4) The use of antipsychotics, and 5) Non-participating in exercises for at least 2 meetings.
Yale Global Tic Severity Scale
The Yale global tic severity scale is a clinician-rated measure for tic severity over the last 7–10 days that has a stable factor structure and excellent psychometric properties. The motor and tics are rated at a 0–5 scale across 5 dimensions: number, frequency, intensity, complexity, and interference [14].
Exercise intervention
The exercise sessions were carried out after school and were conducted in consecutive sessions. Children were transported by bus to a training place in Kermanshah City. Instructors included master’s level physical educators, bachelor’s level exercise scientists, and other trained research staff who had at least some college education. In this study, we emphasized enjoyment and safety but no competition. The aerobic training program was designed using a cycle ergometer, triplicated a week, for 12 weeks, and for an initial period of 40 minutes [16]. The anaerobic training was performed using the method of “Interspaced Training [15]. In this study, parents completed Spence Children’s Anxiety Scale Child and Parent Versions in the pre-test (pre-interventions) and post-test (after 12-week exercises). The questionnaire included 38 items rated on a 4-point scale (0 to 3; never to always), and the SCAS-C includes six additional positive filler items. The SCAS-C/P comprises six subscales addressing Separation Anxiety (six items), Generalized Anxiety (six items), Social Phobia (six items), Obsessive–Compulsive Behaviors (six items), Panic and Agoraphobia (nine items), and Physical Injury Fears (five items).
Statistical Analysis
The present study was conducted in a 2×3 factorial arrangement with the effect of time (pre-test & post-test) and exercises (Control, Aerobic & Anaerobic) and their interaction. The data were reported as mean±SD and analyzed for the main effects of time and exercise and the interactions between time and exercise. The data were analyzed using SPSS 23 software. Comparisons between groups were conducted by the Sceffe test, and the T-test conducted paired-tests. Kolmogorov-Smirnov test was used to test the normality.
Figure 1. Flowchart of the study
Findings
Descriptive characteristics
There were no significant differences between groups (p>0.05) according to age, weight, height, and BMI conditions.
Table 1. The subjects' characteristics
Yale Global Tic Severity Scale
Table 2 presents our findings for five dimensions in the different groups. The results did not show significant differences between groups (p>0.05).
Table 2. Distribution of Yale global tic severity scale scores across participants
Normality
Table 3 shows the normality distribution results for all the parameters in the pre-test and post-test. The results showed that values higher than 0.05 meant normality.
Table 3. The results for normality status (all were normal)
The effect of aerobic and anaerobic fitness on Separation Anxiety
The effect of aerobic and anaerobic fitness on Separation Anxiety for time (F(1, 44)=7.10; p=0.0009), fitness (F(2, 44)=5.41; p=0.001) and time × fitness interaction (F(1, 44)=6.12; p=0.001) were shown in Table 4. Scheffe test showed a significant difference between groups in the post-test (p=0.0001). The results showed that aerobic and anaerobic fitness decreased separation anxiety in the post-test (Table 4).
Table 4. The effect of aerobic and anaerobic fitness on Separation Anxiety in pre and post-Test
The effect of aerobic and anaerobic fitness on Panic and Agoraphobia
The effect of aerobic and anaerobic fitness on Panic and Agoraphobia for time (F(1, 44)=7.08; p=0.0001), fitness (F(2, 44)=7.22; p=0.0001) and time × fitness interaction (F(1, 44)=7.67; p=0.0001) were shown in Table 5. There was a significant response for the Scheffe test in the post-test (p=0.0001). The results showed that aerobic and anaerobic fitness reduced Panic and Agoraphobia (Table 5).
Table 5. Effect of Fitness on Panic and Agoraphobia in pre and post-Test
The effect of aerobic and anaerobic fitness on Physical Injury Fears
The effect of aerobic and anaerobic fitness on Physical Injury Fears for time (F(1, 44)=31.48; p=0.0001), fitness (F(2, 44)=15.48; p=0.0001) and time × fitness interaction (F(1, 44)=16.39; p=0.0001) were shown in Table 6. Scheffe test showed a significant difference between groups in the post-test (p=0.0001). Aerobic and anaerobic fitness decreased Physical Injury Fears (Table 6).
Table 6. Effect of skill exercises on Physical Injury Fears in pre and post-Test
The effect of aerobic and anaerobic fitness on Generalized Anxiety
The effect of aerobic and anaerobic fitness on Generalized Anxiety for time (F(1, 44)=14.20; p=0.0001), fitness (F(2, 44)=21.18; p=0.0001), and time × fitness interaction (F(1, 44)=15.49; p=0.0001) were shown in Table 7. There was a significant response for the Scheffe test in the post-test (p=0.001).
Table 7. The effects of skill exercises on Generalized Anxiety in pre and post-Test
The effect of aerobic and anaerobic fitness on Social Phobia
The effect of aerobic and anaerobic fitness on Social Phobia for time (F(1, 44)=19.60; p=0.0001), fitness (F(2, 44)=21.45; p=0.0001), and time × fitness interaction (F(1, 44)=23.12; p=0.0001) were shown in Table 8. Significant responses were observed for the Scheffe test in the post-test (p=0.0001).
Table 8. The effects of skill exercises on aerobic and anaerobic fitness on Social Phobia in pre and post-Test
The effect of aerobic and anaerobic fitness on Obsessive–Compulsive
The effect of aerobic and anaerobic fitness on Social Phobia for time (F(1, 44)=21.20; p=0.0001), fitness (F(2, 44)=23.31; p=0.0001), and time × fitness interaction (F(1, 44)=19.75; p=0.0001) were shown in Table 9. Significant responses were observed for the Scheffe test in the post-test (p=0.0001).
Table 9. The effects of skill exercises on aerobic and anaerobic fitness on Obsessive–Compulsive in pre and post-Test
Discussion
The results showed that aerobic and anaerobic fitness had positive effects on decreasing psychological disorders in children with tic syndrome. No study has been found to show the effects of aerobic and anaerobic fitness on psychological parameters in children with motor tics. Conversely, Strohle et al. [16] assessed the effects of aerobic treadmill exercise on anti-panic and anxiolytic activity in patients with panic disorder and showed that anxiety was significantly higher in patients submitted to treadmill exercise. The results are in contrast with our findings. The reason for the difference between our findings and others could be attributed to physiological conditions. Parallel to our findings, Bandelow et al. [17] aerobic exercise decreased anxiety symptoms. In another study, Gomes da Silva [18] showed that physical activity affects attention, depression, anxiety, and overall well-being. Other studies showed that aerobic and anaerobic fitness improved neuropsychological and electrophysiological performances of working memory in preadolescent children [19]. An animal study assessed the effects of long-term wheel running on anxiety-like behavior in transgenic mice and showed decreased anxiety-like behavior [20]. It was reported that aerobic exercises have positive effects on the density of neural conveyors in the neural system and reduce muscular tension and hormone levels [20-25]. Other studies showed that aerobic exercises decrease the level of stress and anxiety by influencing the automatic neural system and decreasing anxiety and depression [25]. Aerobic fitness decreases cortisol levels and anxiety [26]. Kim et al. [27] investigated the responses of five participants to aerobic exercises and anaerobic exercises and showed that different fitness improved mental health and happiness, each with a different degree, which verifies the results of the present study. Other studies showed that aerobic and group activities are more effective for improving mental well-being compared to anaerobic and individual exercises [25].
Conclusion
Both fitness similarly decreased psychological disorders in children with tic syndrome. It can be suggested to use aerobic and aerobic fitness to decrease psychological disorders in patients with psychological disorders.
Acknowledgments: This work was supported by Islamic Azad University, Kermanshah Branch, Kermanshah, Iran.
Ethical Permission: None declared by the authors.
Conflicts of Interests: None declared by the authors.
Funding/Support: None declared by the authors.
Article Type: Original Research |
Subject:
Biotechnology
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |